America has two kinds of execution. One is called a death sentence. The other is called compassion. Both use the same drug.
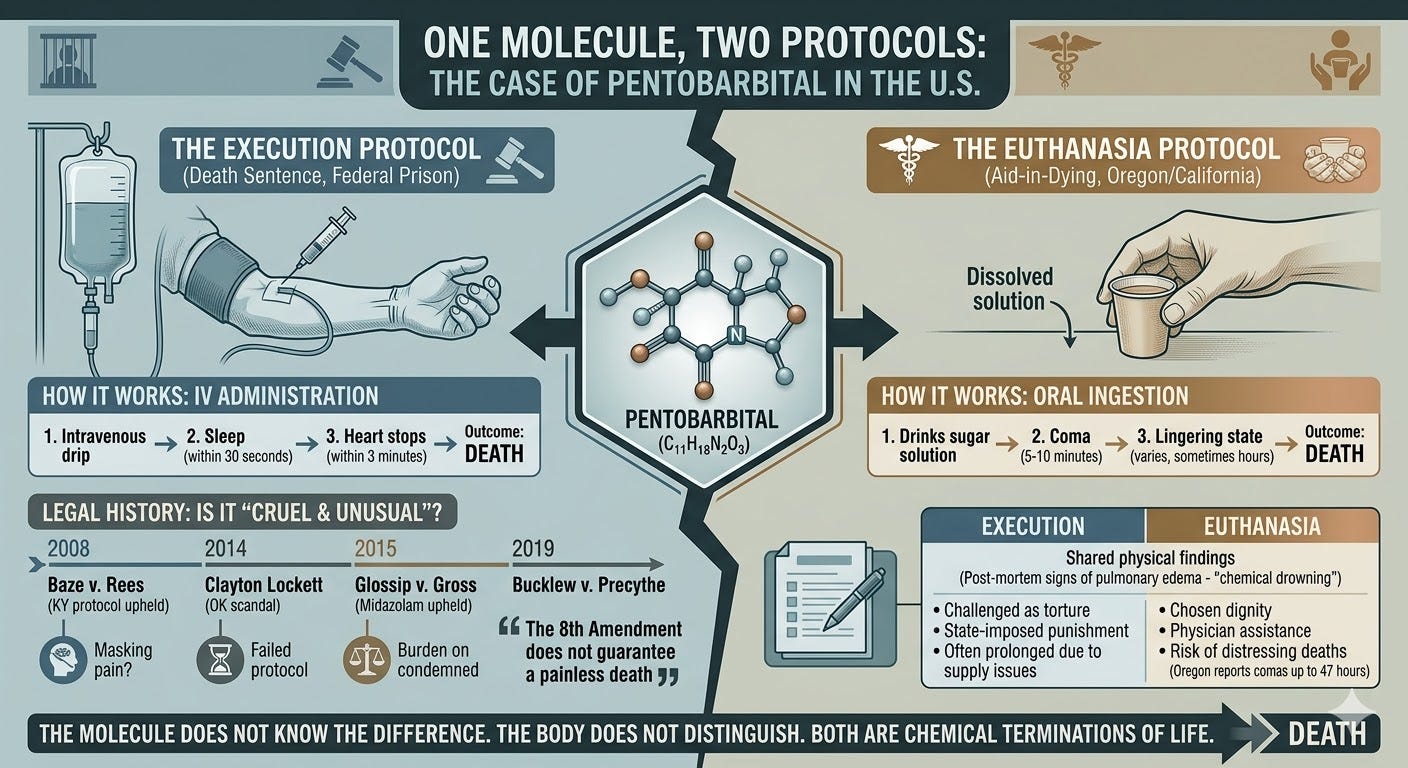
Pentobarbital. It flows into the veins of death row inmates in federal prisons. It gets dissolved into sugar syrup and handed to terminal patients in Oregon and California. Same chemical. Same outcome. Different press releases.
The “Death with Dignity” crowd does not want you to make this connection. They will tell you, loudly, that one execution is forced and one is chosen. That one is punishment and one is mercy. Fair enough. But the molecule does not know the difference, and neither does the body it stops.
How It Works
Administer pentobarbital intravenously and sleep comes within 30 seconds. The heart stops within three minutes. Orally, the patient drinks a solution, falls into a coma within five to ten minutes, and dies. Oregon’s standard euthanasia protocol prescribes 10 grams. Switzerland had to raise its execution dose to 15 grams after some patients lingered in comas for up to 10 hours on lower amounts.
Clean. Clinical. Bilateral.
The Court Said It Might Be Torture
Before we get to the supply chain, we need to sit with the legal history. Because for years, death row inmates and their attorneys argued in federal court that this method of execution was, in the plain language of the Constitution, cruel and unusual punishment.
They had a point.
The three-drug protocol used in most American executions was first seriously challenged in Baze v. Rees, which reached the Supreme Court in 2008. It was the first time in more than a century that the Court examined whether a specific execution method violated the Eighth Amendment. The inmates argued that the paralytic agent in the cocktail, pancuronium bromide, could mask the agonizing effects of the third drug, potassium chloride, leaving a conscious person unable to scream while their heart was chemically stopped. Prisoners contended that the protocol could leave inmates conscious and in terrible pain but, due to complete paralysis, unable to alert anyone to their suffering.
The Supreme Court upheld Kentucky’s method 7 to 2, with no single opinion carrying a majority. The win for the state was narrow and uneasy. Justice Stevens, concurring in the judgment, concluded that the death penalty itself was “patently excessive and cruel and unusual punishment.” Justice Ginsburg dissented, arguing the protocol carried an unacceptable risk of severe pain.
Then states ran out of sodium thiopental and switched to pentobarbital. Then they ran out of pentobarbital. Then Oklahoma substituted midazolam, a sedative not designed for surgical anesthesia, as the first drug in its execution protocol. Oklahoma’s euthanasia of Clayton Lockett in April 2014 became a national scandal. Four death row inmates challenged the midazolam protocol in Glossip v. Gross, arguing it would fail to render them unable to feel the pain of the second and third drugs.
The Supreme Court ruled 5 to 4 in 2015 that the prisoners failed to establish a likelihood of success on the merits of their claim. Justice Alito wrote that in order to prevail, the inmates had to identify a known and available alternative method with a lower risk of pain. In other words: you can challenge your euthanasia method, but only if you can hand the state a better way to execute you. That is the law.
Justice Sotomayor’s dissent did not mince words. She characterized death by lethal injection as “the chemical equivalent of being burned at the stake.”
Justice Sotomayor’s dissent did not mince words. She characterized death by lethal injection as “the chemical equivalent of being burned at the stake.”
The logical endpoint came in Bucklew v. Precythe (2019). Russell Bucklew had tumors filled with blood vessels throughout his head and throat. His doctors testified that a standard pentobarbital execution would rupture those tumors, filling his mouth and airway with blood, causing him to choke and suffocate during the lethal injection process. He asked to be executed by nitrogen gas instead. The Court ruled 5 to 4 against him, holding that the Eighth Amendment does not guarantee a painless death.
Read that again. The highest court in the United States, interpreting the constitutional prohibition on cruel and unusual punishment, ruled that the government is not obligated to euthanize you painlessly.
Now Apply That Logic to the Hospital Room
Here is the question nobody in the aid-in-dying movement wants to answer: if the drug that executes death row inmates has been litigated for two decades as a potential instrument of unconstitutional torture, what exactly is being handed to a terminal patient in a paper cup and called dignity?
Opponents of lethal injection argue that a majority of executed prisoners show postmortem signs of pulmonary edema, their lungs filled with fluid weighing several times normal. If the person were aware, the experience could be akin to suffocation or drowning. That finding applies regardless of whether the death certificate says “execution” or “natural causes accelerated by physician assistance.”
A wide variety of lethal drug combinations are now used across jurisdictions for assisted dying, and the prevalence of complications and failures suggests that applicants are at risk of distressing deaths. One Oregon patient survived his own euthanasia, waking from a three-day barbiturate coma and living another two weeks before dying of cancer. In 2019, one person’s execution by prescribed dose took nearly 47 hours to complete. Another took 19 hours. Eight people have regained consciousness after ingesting supposedly lethal amounts.
The Supply Chain Fiasco
In 2011, death penalty opponents revealed that Lundbeck, a Danish pharmaceutical company, was selling pentobarbital to U.S. states for executions, a practice illegal under Danish law. Lundbeck cut off sales to any American entity involved in executions. The EU followed, expanding its regulations on capital punishment products to cover substances usable in lethal injection, restricting the export of both pentobarbital and secobarbital.
The activists won. They also accidentally euthanized the medical aid-in-dying supply chain.
Before 2012, patients could obtain a sufficient lethal dose for around $500. By 2016, prices had inflated to figures upwards of $25,000. By 2020, Oregon reported that pentobarbital had been unavailable for assisted suicide since 2015, and secobarbital since 2019. States began cobbling together untested execution cocktails, combinations of diazepam, digoxin, morphine, and cardiac drugs, sometimes with results that dragged on for hours.
The Bottom Line
The Supreme Court has spent twenty years being asked whether lethal injection is too cruel for convicted murderers. Its answer, each time, has been: probably not, but we are not entirely sure, and the burden is on the condemned to prove otherwise.
The aid-in-dying movement has spent the same twenty years insisting that the identical pharmacological process is not merely acceptable but humane, dignified, and worthy of legal protection as an expression of personal autonomy.
Both cannot be entirely right. The needle knows no ideology. Pentobarbital does not read the indictment, the diagnosis, or the consent form. It simply executes.
Holding: The Court examined whether the three-drug execution protocol violated the Eighth Amendment's prohibition on cruel and unusual punishment.
